Lip Reconstruction
Your lips are one of the most expressive features of the face. Happiness, sorrow, surprise, and every emotion in between are conveyed through this intricate, mobile structure. More fundamentally, fully functional lips are a prerequisite for normal speech, swallowing, and managing oral secretions — they are not only aesthetic but essential to daily life. Patients with abnormalities or deficits in their lips can gain meaningful improvement with expertly performed lip reconstruction or other lip procedures. Lip reconstruction differs from cosmetic lip enhancement in its central priority: restoring function and natural appearance, rather than refining a normal lip into a different shape.
Lip reconstruction is fundamentally different from cosmetic lip enhancement — the priority is restoring function (speech, eating, oral seal) along with appearance. Dr. Maurice Khosh’s published expertise covers exactly this work. Author of “Lip Reconstruction” — a published chapter through McGraw Hill on the surgical anatomy and aesthetic principles of the lip and perioral region — he is dual board-certified by the American Board of Facial Plastic and Reconstructive Surgery and the American Board of Otolaryngology–Head and Neck Surgery. A Fellow of the American College of Surgeons (FACS), Dr. Khosh holds active hospital privileges at NewYork-Presbyterian, Mount Sinai West, the Manhattan Eye, Ear, and Throat Infirmary (MEETH), and Lenox Hill Hospital — the institutional credentialing required for complex lip reconstruction work.
Conditions Requiring Lip Reconstruction Surgery
Many different conditions can produce the need for lip reconstruction, each requiring a different surgical approach:
- Congenital Malformations (Cleft Lip): Children born with cleft lip require initial surgical repair within the first few months of life, with secondary aesthetic refinements often performed in later childhood and adolescence
- Traumatic Injuries: Lacerations, animal bites, sports injuries, and accidents involving the lip must be treated expeditiously to preserve function and minimize permanent disfigurement
- Cancer-Related Reconstruction: Removal of cancerous lesions of the lip — most commonly squamous cell carcinoma — requires reconstruction as an integral part of overall cancer treatment management
- Facial Nerve Paralysis: Loss of motor function to the lip from stroke, Bell’s palsy, trauma, or surgical complication interferes with speech, swallowing, and the ability to manage oral secretions
- Burn Injuries: Thermal or chemical burns to the lip can produce contracture, distortion, and functional impairment requiring reconstruction
- Revision of Prior Reconstruction: Patients with results from previous lip surgery that did not heal properly or did not adequately restore function or appearance
The Functional Impact of Lip Deformities
For patients with significant lip deformities — particularly those caused by facial nerve paralysis or extensive cancer resection — the functional consequences extend well beyond cosmetic concern. Inability to form a complete lip seal interferes with speech sounds (particularly the “p,” “b,” and “m” sounds that require lip closure), affects swallowing efficiency, and may compromise the ability to manage oral secretions in everyday life. These functional losses often exacerbate the psychological impact of the visible deformity. Successful lip reconstruction must address both dimensions — the visible appearance and the underlying functional capabilities — to truly improve the patient’s quality of life.
“Lip reconstruction is one of the few areas of facial plastic surgery where the goal is not refinement — it’s restoration. Restoring lip closure, speech, the ability to eat without difficulty, and an appearance the patient is comfortable with in social settings. The hierarchy of priorities is functional first, aesthetic second, and the surgical plan reflects what the patient needs most.” — Dr. Maurice Khosh
Lip Reconstruction Techniques: From Simple Repair to Tissue Transfer
The right surgical approach depends on the nature and extent of the deformity. Dr. Khosh draws on a comprehensive range of reconstructive techniques:
- Direct Closure: For smaller defects, the surrounding lip tissue can be carefully advanced and closed with meticulous suture technique
- Local Flaps: Tissue from the adjacent lip or surrounding area rotated, advanced, or transposed into the defect to provide natural color, texture, and function
- Composite Flaps: Combined skin, muscle, and mucosa flaps that restore not just the surface but the underlying muscular function of the lip
- Cross-Lip Flaps (Abbe and Estlander Flaps): Established techniques that transfer tissue from the opposite lip to reconstruct larger defects
- Free Flap Reconstruction: For very large defects involving most of the lip, microsurgical transfer of tissue from a distant site of the body
- Multi-Stage Reconstruction: Layered approach for complex cases where the best result requires more than one surgical procedure
For more minor defects, Dr. Khosh uses simpler techniques designed to restore the aesthetic appearance of the lip with minimal disruption to surrounding tissue. For larger or more functionally significant defects, more involved tissue transfer techniques may be necessary — and Dr. Khosh’s experience across the full reconstructive spectrum allows him to match the right technique to each patient’s specific anatomy and needs.
Multi-Specialty Coordination for Lip Reconstruction
Comprehensive lip reconstruction often requires coordination across multiple specialties. Dr. Khosh works closely with cancer surgeons (particularly head and neck oncologists), dentists and orthodontists, speech and swallow therapists, and pediatric specialists when appropriate. This coordinated approach is particularly important for cancer patients, cleft lip patients, and those with facial paralysis — situations where lip reconstruction is one component of a larger treatment plan rather than an isolated procedure.
Why Choose Dr. Khosh for Lip Reconstruction
- Published Lip Reconstruction Authority: Author of “Lip Reconstruction” through McGraw Hill on the surgical anatomy and aesthetic principles of the lip and perioral region
- Hospital Privileges Across Major Institutions: NewYork-Presbyterian, Mount Sinai West, MEETH, and Lenox Hill — institutional credentialing required for complex reconstructive work
- Full Range of Techniques: From direct closure to local flaps, composite flaps, cross-lip flaps, free flaps, and multi-stage reconstruction
- Function-First Approach: Surgical planning prioritizes speech, swallowing, and oral seal alongside appearance
- Multi-Specialty Coordination: Established working relationships with cancer surgeons, dental specialists, speech therapists, and pediatric teams
- Park Avenue Convenience: Private Upper East Side practice serving patients from across Manhattan and the tri-state area
Schedule Your Lip Reconstruction Consultation in NYC
If you or a family member has been affected by a lip deformity — whether congenital, traumatic, cancer-related, or the result of facial paralysis — the first step is a thorough evaluation of the existing tissue and an individualized surgical plan. Contact us today to schedule a consultation with Dr. Khosh at his Park Avenue office in New York City, or call (212) 339-9988.
Case Studies
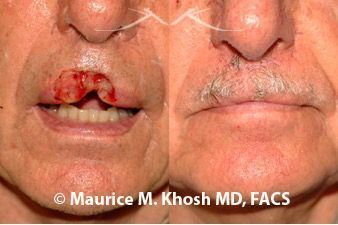
Missing upper middle lip
This 65 year-old-man had cancer removal from the upper middle lip with a full thickness defect of the lip. The lip cancer was removed with the Mohs technique. In repairing the defect, Dr. Khosh advanced the lip edges and hid the scar imperceptibly, to restore the function and aesthetics of the lip.
- Patient: 65 year-old-man with lip cancer
- Problem: Missing upper middle lip
- Procedure: Bilateral advancement flaps

Missing 70% of lower lip
This 71 year-old-woman had cancer involvement of the majority of the lower lip. Dr. Khosh used the two-staged Abbe-Estelander flap (lip switch flap) to move some tissue form the upper lip to the lower lip. The scar in the lips is well hidden, and lip function was restored.
- Patient: 71 year-old-woman with lip cancer
- Problem: Missing majority of lower lip
- Procedure: 2 staged Abbe-Estlander flap (lip switch flap)

Missing lower lip lining
This 69 year-old-man had basal cell cancer of lower lip. The cancer was removed with Mohs technique. The red part of the lip was missing with intact underlying muscle. Dr. Khosh used a mucosa flap (the lining of the mouth) from inside the mouth to provide a good match to the normally red part of the lip.
- Patient: 69 year-old-man with lip cancer
- Problem: Missing lower lip with intact underlying muscle
- Procedure: Mucosal flap (transfer of the lining of the mouth)

Missing 1/3 of lower lip
This 45 year-old-man had basal cell cancer of lower lip. Cancer was removed with Mohs technique. Dr. Khosh advanced the intact edges of the lip to restore normal lip function. The length of the scar was limited by using a technique known as “M-plasty”.
- Patient: 45 year-old-man with lower lip cancer
- Problem: Missing muscle and lining of the lower lip
- Procedure: Advancement flap and M-plasty
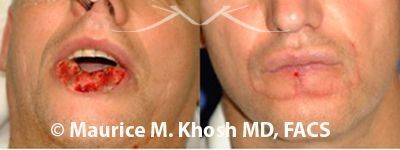
Missing entire lower lip
This 52 year-old-man had squamous cell cancer of the lower lip. During Mohs surgery for cancer removal, nearly all the lower lip was removed. Dr. Khosh used a special surgical technique, known as a Karapandzic flap, to mobilized tissue around the mouth allowing closure of the lip. The post op picture was taken one week after surgery.
- Patient: 52 year-old-man with lip cancer
- Problem: Missing entire lower lip
- Procedure: Karapandzic flap

Small defect of upper lip near nose
This 51 year-old-woman had a basal cell cancer of upper lip near the nose. Mohs surgery resulted in an 8-mm circular defect near the nose. Dr. Khosh repaired this with local tissue advancement to hide the scar at the junction of the lip and the nose.
- Patient: 51 year-old-woman with cancer of the lip
- Problem: 8-mm defect near the nose
- Procedure: Local tissue advancement
Disclaimer: These are actual results for patients of Dr. Maurice Khosh. Plastic and cosmetic surgery results can vary between patients.
Frequently Asked Questions
-
This is dependent on the nature of reconstruction. Small procedures for lip reconstruction such as local flaps and direct closure can be performed as an office procedure under local anesthesia. More complicated procedures involving large lip defects commonly require sedation or general anesthesia in an operating room.
-
Whistle lip deformity is a central notching of the upper lip following repair of a cleft lip, or following repair of a central upper lip defect. It is due to missing soft tissue. Repair can be accomplished with small local flaps, or with injection of filler agents such as Restylane or Juvederm.
-
The Abbe Estelander flap is a lip switch technique in which a defect of the upper lip is repaired with tissue borrowed from the lower lip, and vice versa. It is ideal for lip defects that involve more than half of the lip. The Abbe Estelander flap is performed in two stages that are separated by two or more weeks.
-
When a lip defect involves more that 75% of the lip, the Karapandnzic flap can be used for repair. Circular flaps from around the mouth are used to repair the defect. The Karapandnzic flap preserves the nerve and vascular supply of the residual lip, and allows immediate lip function.
-
The Karapandnzic flap can be used for lip repair when the defect is greater than 75% of the lip. Circular flaps from around the mouth are used to repair the defect. The Karapandnzic flap preserves the nerve and vascular supply of the residual lip, and allows immediate lip function.
Related Procedures
Lip reconstruction for traumatic, congenital, or cancer removal aims at restoring the function and appearance of the lips. The procedures are typically not associated with other facial treatments. Occasionally, laser treatments are used to help camouflage skin scars.