Cheek Reconstruction Surgery
Cheek reconstruction is among the most challenging applications of facial plastic surgery — the cheek is a highly visible feature of the face, and rebuilding it after cancer removal, traumatic injury, or congenital anomaly demands both technical surgical precision and the aesthetic judgment to restore a natural appearance. The most common reason patients require cheek reconstruction is Mohs surgery for skin cancer, which removes the cancerous tissue but leaves a defect that needs to be closed using surrounding skin, local tissue flaps, skin grafts, or, in larger cases, tissue expansion techniques. Other patients require reconstruction after trauma, burns, or surgical excision of larger tumors. Cheek reconstruction is one of the reconstructive options for the face and neck at Dr. Khosh’s Park Avenue practice in New York City.
Dr. Maurice Khosh’s published reconstructive expertise is directly relevant to cheek reconstruction work. He authored “Surgical Treatment of Facial Scars” — a chapter through Thieme Publishers — and has published additional reference work on tissue expansion, the technique used to grow extra skin for closure of larger defects. Dual board-certified by the American Board of Facial Plastic and Reconstructive Surgery and the American Board of Otolaryngology–Head and Neck Surgery and a Fellow of the American College of Surgeons (FACS), he holds active hospital privileges at NewYork-Presbyterian, Mount Sinai West, the Manhattan Eye, Ear, and Throat Infirmary (MEETH), and Lenox Hill Hospital — the institutional credentialing required for the surgical settings reconstructive work demands.
When Cheek Reconstruction Is Needed
Dr. Khosh performs cheek reconstruction for a range of indications, each requiring an individualized surgical plan:
- Mohs Skin Cancer Reconstruction: Closure of the defect left after dermatologic surgeons remove basal cell, squamous cell, or melanoma skin cancers from the cheek
- Traumatic Injury Repair: Reconstruction following lacerations, abrasions, animal bites, or vehicle accidents
- Burn Reconstruction: Restoration of cheek contour and skin quality following thermal or chemical injury
- Tumor Resection Defects: Closure following removal of benign or malignant tumors of the soft tissue, parotid gland, or facial bone
- Congenital Anomalies: Repair of cheek deformities present from birth, such as facial clefts or hemifacial differences
- Revision Cases: Improvement of unsatisfactory results from previous reconstructive attempts
Reconstructive Techniques
Each cheek reconstruction is individually planned based on the size and location of the defect, the surrounding tissue available for use, and the patient’s overall goals. Dr. Khosh draws on a broad range of reconstructive techniques:
- Local Flaps: Surrounding skin and underlying tissue rotated, advanced, or transposed into the defect to provide both coverage and natural blood supply
- Skin Grafts: Thin layers of skin transferred from another part of the body to cover the defect when local flaps are not feasible
- Tissue Expansion: A staged technique in which a small inflatable expander is placed beneath nearby skin to gradually grow additional tissue for closure of larger defects
- Composite Grafts: Combined skin and underlying tissue grafts used in selected cases requiring more substantial replacement
- Free Flap Reconstruction: For very large or full-thickness defects, transferring tissue (sometimes with its own blood supply) from a distant body site
- Multi-Stage Reconstruction: Layered approach for complex cases where the best result requires more than one surgical procedure
“Cheek reconstruction is judgment-driven work. Every defect is different — the size, the depth, the location relative to the eyelid and lip, the quality of the surrounding tissue. The reconstructive options available range widely, and matching the right technique to the specific defect is what determines whether the result blends in or stands out.” — Dr. Maurice Khosh
A Multi-Stage Approach for Complex Cases
While many cheek defects can be reconstructed in a single procedure, larger or more complex cases sometimes require a staged approach. This may involve an initial reconstruction followed by scar revision, tissue expansion followed by flap closure, or several smaller refinements that together produce the most natural-appearing final result. Dr. Khosh discusses the timeline and reasoning for each stage in detail during consultation, ensuring patients understand the full plan before the first procedure begins.
Why Patients Choose Dr. Khosh for Cheek Reconstruction
- Published Reconstructive Authority: Author of chapters on facial scar treatment and tissue expansion — the techniques most often used in cheek reconstruction
- Hospital Privileges Across Four Major Institutions: NewYork-Presbyterian, Mount Sinai West, MEETH, and Lenox Hill
- Dual Board Certification: Both facial plastic and head and neck surgery expertise relevant to reconstructive work
- Full Range of Techniques: Local flaps, grafts, expansion, and multi-stage approaches selected based on the specific defect
- Park Avenue Convenience: Private Upper East Side practice serving patients from across Manhattan and the tri-state area
Schedule Your Consultation in Manhattan
Whether you have recently completed Mohs surgery, sustained a traumatic injury, or are seeking improvement after a previous reconstruction, the right outcome depends on detailed evaluation of the existing defect and an individualized plan tailored to your anatomy and goals. To schedule a consultation with Dr. Khosh at his Park Avenue office in New York City, call (212) 339-9988 or contact us online to request an appointment.
Case Studies
Please view the case studies listed below for examples of cheek reconstruction for various deformities including skin defects, cheekbone fractures, or congenital deformities.


Skin defect in middle of cheek
This 35 year-old-female has Mohs excision of a basal cell cancer from the middle of her cheek, resulting in a 2.5 x 1.5 cm loss of skin. Repair under local anesthesia resulted in an imperceptible scar.
- Patient: 35 year-old-female with skin cancer
- Problem: 2.5 x 1.5 cm mid cheek skin defect
- Procedure: Flap repair of cheek defect


Skin defect of cheek in front of ear
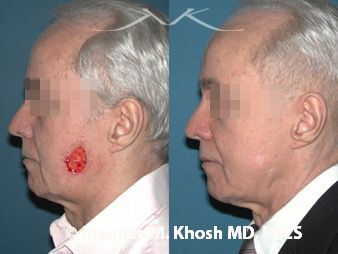
This 38 year-old-female has had multiple basal cell cancers of the face. Removal of a recurrent cancer resulted in a 5.5 x 3.5 skin loss in front of the ear. A facelift type flap was used to move the cheek skin back and hide the resultant scar.
- Patient: 38 year-old-female with skin cancer
- Problem: 5.5 x 3.5 cheek skin defect in front of the ear
- Procedure: Facelift flap to cover the defect and hide the scar


Skin defect at junction of the cheek and lip
This 66 year-old-female had a basal cell cancer removed by Mohs surgery. There was a 1.75 cm skin defect at the junction of the cheek and upper lip. An island pedicle flap was used for repair. The scar lines are well hidden in the natural creases of the face.
- Patient: 66 year-old-female with skin cancer
- Problem: 1.75 cm skin defect of cheek near the upper lip
- Procedure: Island pedicle flap


Congenital under development of cheek
This 38 year-old-male was born with congenital under development of the left side of his face. Ten years ago, a cheek implant was placed in hopes of improving the facial appearance. The entire left side of the face was augmented with two sessions of fat grafting.
- Patient: 38 year-old-male
- Problem: Under developed left cheek and face
- Procedure: Fat grafting in two sessions

Skin defect of cheek near the temple
This 57 year-old-female had a basal cell cancer removed from the upper-outer cheek near her temple. She had a large circular defect measuring 3.5 cm in diameter. This was repaired with a cheek advancement flap with an imperceptible scar.
- Patient: 57 year-old-female with skin cancer
- Problem: 4.5 cm defect of upper outer cheek
- Procedure: Cheek advancement flap
Skin defect of the lower-outer cheek
This is a 56 year-old-male after removal of basal cell cancer in the lower-outer part of cheek. This resulted in a 4.0 x 3.5 cm defect of the skin. The area was repaired with a rhombic transposition flap.
- Patient: 56 year-old-male with skin cancer
- Problem: 4.0 x 3.5 cm skin defect in the lower-outer cheek
- Procedure: Rhombic transposition flap
Disclaimer: These are actual results for patients of Dr. Maurice Khosh. Plastic and cosmetic surgery results can vary between patients.
Frequently Asked Questions on Cheek Reconstruction
-
Repair of small and medium sized cheek skin cancer defects and cheek augmentation with fat transfer can be performed under local anesthesia. Surgical repair of larger cheek defects and repair of cheek fractures requires general anesthesia in an operating suite.
-
The swelling and bruising that follows surgical repair of cheek skin cancer defects or cheek fractures is mostly resolved after two weeks. Most patients can return to work at that time.
-
In most cases, sutures are removed after 5 to 7 days.
-
Advancement flaps are quite useful in repair of cheek defects. The skin from the remaining, intact cheek is advanced to the site of the defect, and the incisions are closed. This requires additional incisions on the face, but such incisions heal quite well.
Related Procedures
Reconstructive surgery for cheek defects is aimed at restoring the face. In skin cancer repair, related procedures may entail secondary surgical treatments to enhance the cheek appearnce or laser treatments to camouflage scars. In facial fracture repair, related procedure may include fat transfer or facial filler injections to improve facial contours.

Click Here to See Cheek Photo Gallery